Gynecomastia (enlargement of the male breast secondary to an increase in glandular tissue and stroma) can be a vexing clinical problem.1-3 Often, it is a benign finding, but sometimes it is an important clue to disease elsewhere4 (Table 120-1). Thus, the condition cannot be dismissed as a simple cosmetic defect, although, in a substantial number of cases no underlying cause is ever found.
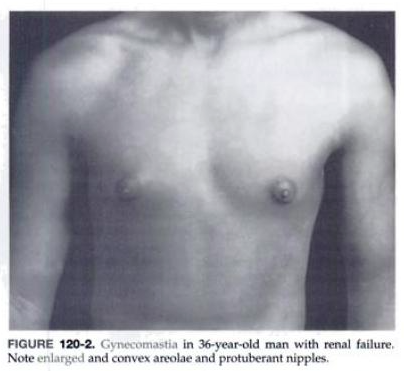
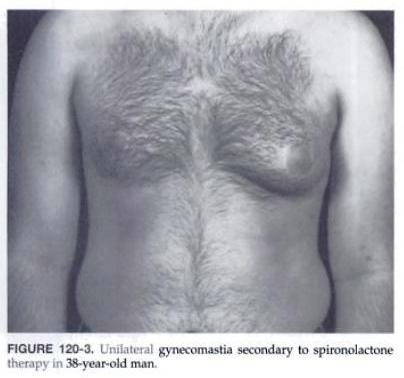
On physical examination, it is necessary to distinguish between psuedogynecomasatia, which is breast enlargement caused by increased adipose tissue, and true gynecomastia (Fig. 120-1). In the latter condition, there is an enlargement of the mammae. The glandular tissue can be palpated as radially arranged cords, usually around the nipple, and may form a discrete button-like mass or merge gradually with the surrounding adipose tissue. The areolae may be enlarged and convex, and the small areolar glands (glands of Montgomery) often are prominent. Frequently, the mammary papilla or nipple is enlarged and protuberant (Fig. 120-2). Breast tenderness (mastodynia) may be present, particularly if the onset is recent. Although commonly bilateral and symmetric, gynecomastia of any cause may be unilateral or markedly asymmetric, either initially or throughout its course (Fig. 120-3).
Histologically, there may be hyperplasia of the epithelial or stromal cells or an increase in fibrous tissue. The appearance tends to correlate with the duration of the condition. Thus, gynecomastia of more recent onset tends to show cellular hyperplasia that, over time, progresses to increased fibrous tissue without increased cellularity, including new induction of type VI collagen. This increase in fibrous tissue explains why long-standing gynecomastia is so difficult to treat by nonsurgical means.
Because so many conditions can cause gynecomastia, it is not unusual to encounter the condition clinically. In addition, several studies have reported a high prevalence of gynecomastia in the normal population (>40% of young, healthy men) and in hospitalized patients.1 Often, gynecomastia represents the quiescent residual enlargement attributable to a condition that is no longer present.
Given the long recognized role of estrogens in stimulating mammary growth, it is not surprising that high circulating estrogen levels of exogenius or endogenious origin can be associated with gynecomastia. More recently, however, gynecomastia has been noted in disorders with deficient androgen production even when estrogen production is normal, leading to the concept that gynecomastia often maybe related to increases in the circulating estrogen/androgen ratio rather than to absolute increases in estrogen per se. Finally, the occurrence of gynecomastia in conditions in which the androgen insensitivity of peripheral target tissues is reduced, even without significant changes in circulating androgens or estrogens, has refined this concept to suggest that gynecomastia is related to the resultant estrogen/androgen ratio affect at the breast. Although experimental evidence is inconclusive, this has proved to be a useful framework for evaluating gynecomastia.
In men, the principle circulating androgenic activity resides in testosterone, which originates almost exclusively from testicular secretion. By contrast, the major estrogenic affect in man is related to circulating estradiol and estrone, most of which originated from the conversion of circulating androgenic precursors to estrogens by peripheral tissue such as fat. Because a substantial fraction of these androgen precursors is of adrenal origin, and endocrine dysfunction limited to the testis can cause significant reductions in circulating androgens with less effect on circulating estrogens, and the resulting increase in the estrogen/androgen ratio can lead to gynecomastia. This general scheme is thought to apply in a variety of testicular disorders.
Primary increases in estrogen production also have secondary effects that can further elevate the estrogen/androgen ratio and enhance gynecomastia: stimulation of sex hormone-binding globulin (SHBG) levels or suppression of androgen production by direct inhibition of testicular biosynthetic enzymes or by inhibition of leutinizing hormone (LH). Increased activity of the enzyme aromatase, which converts androgens to estrogens, has been noted in tissues from some patients with gynecomastia, suggesting that local production of estrogen within the breast may also Play a contributory role.
In addition to the role of androgens and estrogens, the role of gonadotropins in relation to gynecomastia needs to be considered. LH and human chorionic gonadotropin (hCG) increase the secretion of estradiol from Leydig cells in the testis; therefore, gynecomastia is particularly common in forms of testicular dysfunction in which circulating gonadotropin levels are elevated (primary testicular failure). Conversely, gynecomastia is less common when testicular dysfunction is accompanied by low circulating gonadotropin levels, as may occur in some pituitary disorders. Also, in the latter condition, coexistent impairment of adrenocorticotropic hormone (ACTH) release may decrease the adrenal output of the androgens that serve as precursors for circulating estrogens, thus decreasing further the estrogen/androgen ratio.
Hyperprolactinemia, which is implicated strongly in galactorrhea (milky breast discharge), rarely is a cause of gynecomastia. However, disorders causing increases in the circulating estrogen/androgen ratio may result in both hyperprolactinemia and gynecomastia as independent secondary effects. In addition, a patient with hyperprolactinemia may have gynecomastia from secondary hypogonadism consequent to the prolactin excess or from another cause totally unrelated to the hyperprolactinemia. Galactorrhea appears more likely to occur in a hyperprolactinemic man who happens to have concurrent gynecomastia.
{kind=link}
{kind=link}
{kind=link}
{kind=link}